

Most denials are not caused by incorrect coding. They are caused by missing or insufficient justification.
Medical necessity is the standard that determines whether a service will be reimbursed. And that standard is evaluated entirely through documentation.
If the documentation does not clearly explain why a service was needed, the claim will not hold up under payer review or audit.
What Medical Necessity Actually Means in Practice
Medical necessity means a service is:
- Clinically appropriate for the patient’s condition
- Supported by objective findings and clinical evidence
- Not performed for convenience
- The most appropriate next step in care
Payers do not reimburse based on what was performed. They reimburse based on what is documented and justified.
The Three Pillars Auditors Expect to See
Every medically necessary service should clearly demonstrate:
Clinical Indication
A clearly documented diagnosis or symptom that justifies the service.
Conservative Treatment (When Applicable)
Evidence that lower-level treatments were attempted first, including:
* Dates
* Duration
* Patient response
Expected Benefit
A clear explanation of how the service will impact diagnosis or treatment decisions.
If any one of these elements is missing, the claim is at risk.
The MEAT Framework: How Auditors Read Your Notes
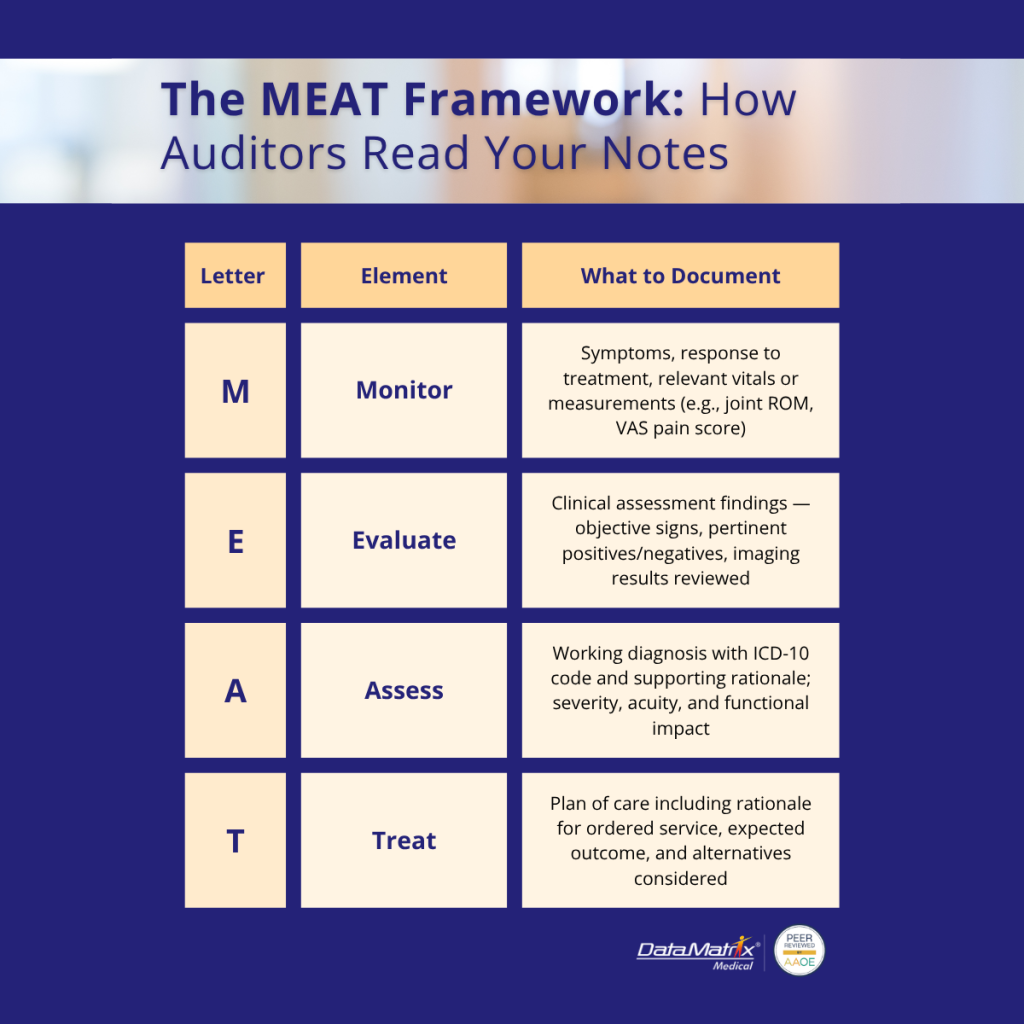
Auditors are not reading for volume. They are reading for structure and clarity.
Strong documentation should include:
- Monitor: Symptoms, progression, response to treatment
- Evaluate: Objective findings, exam results, and imaging reviewed
- Assess: Diagnosis with severity, acuity, and rationale
- Treat: Plan of care, including why the service is being ordered
If your documentation does not follow this logic, it becomes difficult to defend.
Functional Impact: The Most Commonly Missed Element
One of the most common reasons for a prior authorization denial is a lack of functional impact.
It is not enough to document a condition. You must document how it affects the patient’s life.
Example:
- Weak: “Right shoulder pain.”
- Strong: “Right shoulder pain limiting ability to lift overhead and perform job duties.”
Functional language converts clinical findings into a reimbursable justification.

Orthopedic Examples: Where Medical Necessity Often Fails
Knee MRI Denials
A common issue is ordering imaging without documenting conservative care.
Typical elements missing from documentation:
- Duration of symptoms (e.g., “8-week history of worsening right knee pain following a twisting injury, with no improvement after NSAIDs and activity modification”)
- Physical exam findings (e.g., “Positive McMurray test on the right knee, decreased range of motion from 0–90°, joint line tenderness medially, and mild effusion noted on exam”)
- PT or medication trials (e.g., “Completed 6 weeks of physical therapy from Jan–Feb 2026 with minimal improvement in pain and function; trial of NSAIDs and corticosteroid injection provided only temporary relief”)
Strong documentation should include:
- Symptom timeline (e.g., “Patient reports progressive right knee pain over 8 weeks following a twisting injury, initially intermittent but now constant, worsening with weight-bearing and limiting daily activity”)
- Objective findings (ROM, positive tests)
- Failed conservative care (with dates)
- Clear clinical question the MRI will answer (e.g., “MRI of the right knee ordered to evaluate for suspected medial meniscus tear vs. ligament injury and to determine if the patient is a candidate for surgical intervention after failed conservative treatment”)
Rotator Cuff Surgery
Required documentation includes:
- Functional limitation (inability to lift, work restrictions)
- Imaging confirmation
- Failed non-operative management
- Duration of symptoms
Injection Therapy (Cortisone, etc.)
Documentation must show:
- Prior treatment attempts
- Patient response history
- Justification for repeat or continued therapy (e.g., “Patient reports temporary pain relief for 4–6 weeks following prior corticosteroid injection, with recurrence of symptoms impacting ambulation and daily activity; repeat injection indicated to manage inflammation and delay need for surgical intervention”)
Common Medical Documentation Gaps That Trigger Denials
In no particular order, here are the common medical documentation gaps we see that trigger denials:
- Vague or generic language
- Missing timelines
- No documented conservative care
- Lack of functional impact
- Inconsistent notes across visits
- Orders without a clinical rationale
These gaps increase denial rates and create additional administrative burden for staff. This is why we know the importance of medical documentation to medical coding accuracy
How Poor Document Management Increases Audit Risk
Lost or Hard-to-Retrieve Records
If documentation cannot be accessed quickly, it may as well not exist during an audit.
Inconsistent Data Across Systems
Differences between EHR notes, imaging reports, and billing records raise red flags (e.g., the EHR note documents “right knee pain x 2 weeks” with no conservative care, the MRI report references chronic degenerative changes, and the claim is billed with an acute injury ICD-10 code and no documented PT/NSAID trial; or laterality/date mismatches such as “left shoulder” in the note vs. “right shoulder” on the order).
Delayed Documentation
Late entries weaken credibility and make medical necessity harder to defend (e.g., when notes are entered days after the encounter, they often lack precise symptom timelines, objective findings, and real-time clinical reasoning; auditors may view these as reconstructed rather than contemporaneous, making it difficult to prove that the service decision was based on documented evidence at the time of care, which undermines both medical necessity and compliance).
Learn more: Document Indexing Services
Prior Authorization: Where Documentation Is Tested First
Prior authorization is often the first place medical necessity is evaluated.
Strong submissions should include:
- Full clinical notes (not just the order)
- Supporting documentation (imaging, PT notes, labs)
- Clear alignment with payer criteria
Treat every submission as if it will be reviewed by someone unfamiliar with the patient.
How Structured Documentation Improves Approval Rates
Consistent templates, real-time documentation support, and centralized document management ensure that all required elements are consistently captured.
Related: Medical Documentation Explained
The Role of Documentation in Audit Readiness
Strong documentation creates a defensible record that supports billed services.
This reduces:
- Audit exposure
- Recoupments
- Compliance risk
And improves:
- Approval rates
- Revenue predictability
- Efficiencies across the practice
How DataMatrix Medical Supports Medical Necessity Documentation
DataMatrix Medical provides documentation support, prior authorization alignment, and billing coordination to ensure medical necessity is clearly documented and supported. Completely compliant and secure solutions that your IT guy and billing department would approve.
Explore: Medical Billing Solutions
Conclusion
Medical necessity is not assumed. It must be proven through documentation.
Improving documentation processes helps reduce denials, strengthen compliance, and protect revenue. But you know that already.

Nathaniel Smathers is the VP of Client Education and Marketing. He is also a long time contributor of the DataMatrix Medical blog and has a background in healthcare content creation for over a decade. Nathaniel is passionate about exploring the intersections of healthcare, data analysis, and digital innovation.

{kind=link}