

When a claim comes back denied, the instinct is usually the same: send it to billing, figure out what went wrong, and resubmit. That workflow might feel like a system, but for many practices it masks a much larger issue. Prior authorization denials and billing denials are fundamentally different problems with distinct root causes, owners, and resolution paths. Mixing them up costs practices real money.
According to the American Medical Association, physicians and their staff spend an average of 14.9 hours per week, or over 39 prior authorizations per physician, dealing with or fixing prior authorizations. That figure alone tells you the administrative weight these processes carry. But when a practice cannot distinguish between a denial that occurred before the patient was ever seen and one that resulted from how the claim was submitted, that weight becomes heavier and harder to manage strategically.
This guide breaks down both types of denial, explains how to quickly identify them, walks through resolution workflows, and outlines upstream practices to prevent their recurrence.
Two Different Problems, Two Different Solutions
Before diving into workflows, it helps to anchor the core distinction:
Authorization Denial
- A front-end failure
- Occurs before or at the time of service
- Caused by missing, expired, or incorrect authorization
- Often tied to surgical or advanced procedures
- Owned by the authorization and front-desk team
- Preventable before the patient visit
Billing Denial
- A back-end failure
- Occurs during or after claim submission
- Caused by coding errors, data entry issues, or process gaps
- Identified via coding or processing error on the EOB
- Owned by the billing team
- Correctable within the billing workflow
That distinction is not just academic. It determines who needs to be involved in resolution, where your appeal energy should be directed, and what operational changes will actually reduce future denials.
Authorization Denials: A Front-End Problem
An authorization denial occurs when a required prior authorization was not obtained, has expired, or was obtained for the wrong CPT code, provider, or facility. By the time the claim comes back denied, the service has already been rendered. That is what makes this category particularly costly.
Common Causes
In practice, authorization denials tend to cluster around a handful of recurring issues: no authorization on file, an expired authorization, an authorization tied to the wrong CPT code, a service that exceeded the authorized number of units, or an authorization issued for a different provider or facility than the one who actually rendered the service.
Each of these represents a process failure at the front end of the revenue cycle, not the back end. The clinical encounter may have been perfectly documented. The coding may have been textbook. But if the authorization piece was not handled correctly before the appointment, none of that matters to the payer.
11% |
65% |
$25 to $30 |
|---|---|---|
| of healthcare spending is estimated to be lost annually to claim denials and rework, per the Advisory Board | of denied claims are never reworked or resubmitted, leaving revenue permanently on the table | average cost to rework a single denied claim, according to MGMA data |
How to Identify an Authorization Denial
The EOB will typically reference language like “No Authorization on File,” “Precertification Required,” or “Service Not Authorized.” Critically, the rest of the claim will often look clean. No coding issues, no data errors. That combination, a clean claim with an auth-related denial reason, is a reliable indicator that you are dealing with a front-end failure, not something the billing team caused.
Resolution Workflow
The first step is confirming whether an authorization was actually obtained. If it was, the resolution path is relatively straightforward: correct the claim with the proper authorization number and resubmit. If no authorization exists, the practice needs to contact the payer immediately and determine whether a retroactive authorization is available. Not all payers allow retro auth, and those that do typically have strict timelines and criteria. If retro auth is denied, the practice faces a harder conversation: determining whether the cost becomes patient responsibility and documenting all actions taken along the way.
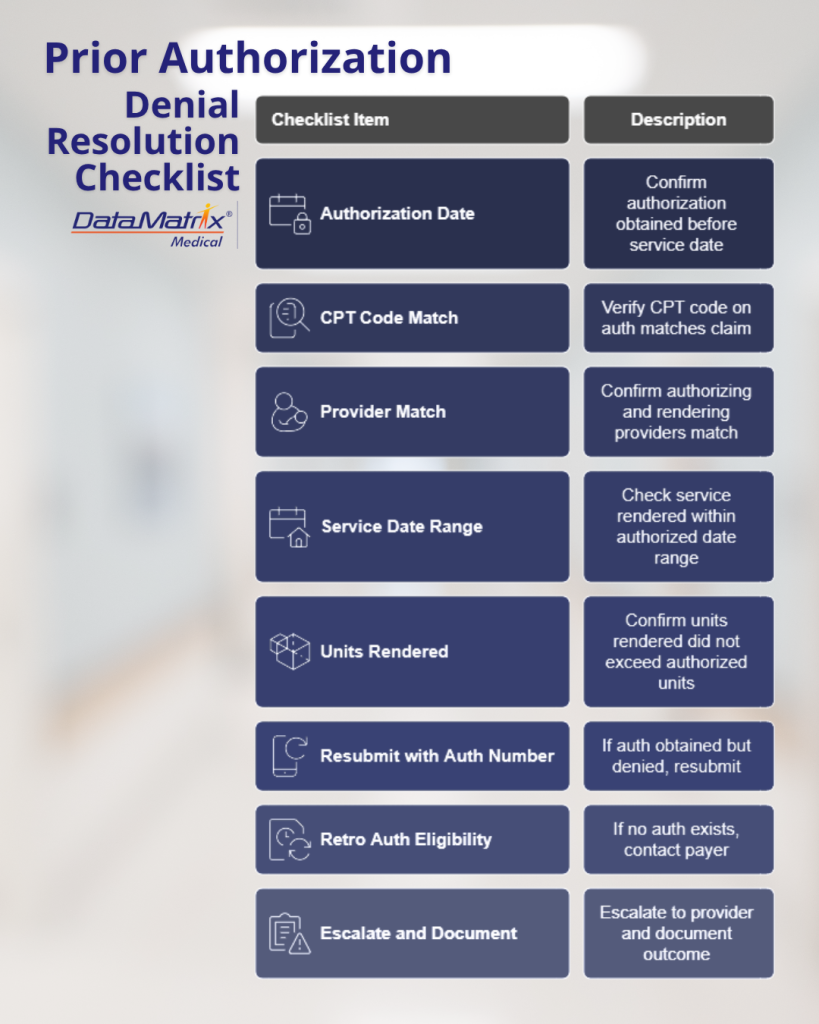
- Confirm whether authorization was obtained before the service date
- Verify the CPT code on the auth matches the CPT code on the claim
- Confirm that the authorizing provider and rendering provider match
- Check that the service was rendered within the authorized date range
- Confirm units rendered did not exceed authorized units
- If auth was obtained but denied, resubmit with the correct auth number
- If no auth exists, contact the payer for retro auth eligibility
- Escalate to the provider and document the outcome if retro auth is denied
Escalation
Authorization denials escalate to the front desk team or the authorization department, not the billing team. Provider involvement may be necessary if a peer-to-peer review is required to support a retro-auth request. Keeping billing out of the resolution loop when it is an auth issue prevents confusion and keeps accountability where it belongs.
Billing Denials: A Back-End Problem
Billing denials occur during or after claim submission and are caused by errors in how the claim was coded or processed. Unlike authorization denials, these are owned entirely by the billing team and resolved within that workflow. They are also among the most correctable types of denials when caught and addressed quickly.
Common Causes
Billing denials cover a wide range of issues: incorrect CPT or ICD-10 codes, missing or inappropriate modifiers, an invalid payer ID, incorrect place of service, duplicate claim submission, a timely filing violation, or a provider not credentialed with the payer being billed. Some of these are data entry errors. Some are process failures. Some are knowledge gaps around payer-specific requirements. But they share a common thread: none of them is tied to whether an authorization was in place.
How to Identify a Billing Denial
The EOB will list a coding or processing error as the denial reason, with no reference to authorization. Common CARC codes in this category include denials for duplicate submissions, invalid billing information, coding errors resulting in non-covered services, and provider enrollment issues. These denials signal that the claim needs to be corrected and resubmitted, not that an authorization needs to be chased.
Resolution Workflow
The billing denial resolution workflow is more linear than its authorization counterpart. Open the claim, review the EOB for the specific denial reason, correct the identified error, whether that is a code, a modifier, payer information, or a credentialing issue, resubmit, and track for acceptance. The key discipline is documenting the correction made, not just the resubmission. That documentation becomes critical when patterns emerge across multiple denials and a practice needs to identify whether a systemic process change is warranted.
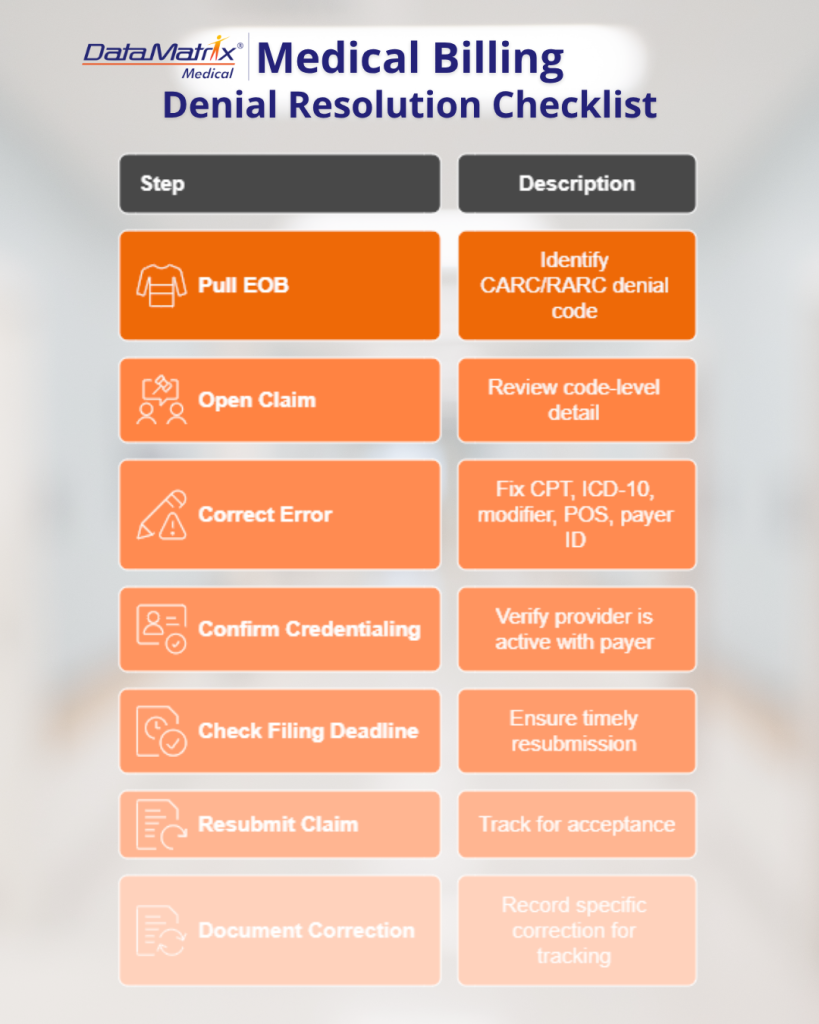
- Pull the EOB and identify the specific CARC/RARC denial code
- Open the original claim and review all code-level detail
- Correct the identified error (CPT, ICD-10, modifier, place of service, payer ID)
- Confirm provider credentialing is active with the billed payer
- Check the timely filing deadline before resubmitting
- Resubmit the corrected claim and track for acceptance
- Document the specific correction made for trend tracking
Escalation
Most billing denials should be resolved within the billing team without escalation. The exception is when a denial requires a coding determination that goes beyond the biller’s scope. In those cases, a coding review or a consultation with the clinical team may be necessary before resubmission. Escalating coding questions rather than making assumptions on the resubmission is a safeguard worth building into any denial workflow.
A Quick-Reference Comparison
| Category | Authorization Denial | Billing Denial |
|---|---|---|
| Where it originates | Front-end (before or during service) | Back-end (claim submission) |
| Primary cause | Missing, expired, or incorrect authorization | Coding or data entry error |
| EOB language | “No Authorization,” “Precertification Required” | Coding error, invalid info, duplicate |
| Claim otherwise clean? | Usually yes | Usually no |
| Who resolves it | Authorization team / front desk | Billing team |
| Preventable upstream? | Yes — before the visit | Yes — before submission |
| Escalation path | Auth team, provider if needed | Billing team; coding if needed |
| Retroactive fix available? | Sometimes (retro auth, payer-dependent) | Yes, via corrected claim |
Why Misclassification Is Costing Your Practice
The operational consequences of confusing these two types of denial are underappreciated. When authorization denials get routed to billing, billers spend time trying to resolve something that is not within their control. Authorization denials often require real-time payer contact, provider involvement, and decisions about patient financial responsibility, none of which a biller should be navigating alone. Meanwhile, the denial ages. Timely filing deadlines approach. Retro auth windows close. Revenue that was recoverable becomes permanently lost.
The reverse problem is equally damaging. When a billing denial is escalated as though it were an authorization issue, it creates unnecessary noise for authorization and front-desk teams, delays resolution, and obscures what is often a straightforward coding fix.
For practice administrators and MSO leaders, this is fundamentally a workflow design problem. The question is not whether your team can eventually resolve these denials. It is whether your process is structured so the right people are working on the right denials from the moment the EOB is received.
Building a Denial Triage System That Works
The most functional denial management systems share one characteristic: they classify before they resolve. Whether that classification occurs through your practice management system, a denial-tracking spreadsheet, or a dedicated RCM platform, the mechanism matters less than the discipline of asking a single question before assigning any denial to a queue.
Does the EOB reference authorization? If yes, it is a front-end issue. Does it reference coding, data, or submission? If yes, it is a billing issue. That decision rule is simple enough to train on and consistent enough to hold up across payers, specialties, and service types.
From there, denial management becomes a matter of clear ownership, documented workflows, and trend data. Practices that track denial reason codes over time can identify whether they have a systemic authorization process gap, for example, a specific service type consistently authorized with the wrong CPT code, versus a billing gap, such as a modifier incorrectly applied to a specific payer’s claims. Those are distinct root causes requiring distinct interventions, and you cannot reach them without classification data.
- Denial references authorization? Treat as front-end. Route to the authorization team. Involve the provider if retro auth or peer-to-peer is needed.
- Denial references coding, data, or submission error? Treat as back-end. Route to the billing team. Escalate only if coding clarification is needed.
Where Documentation Fits In
One factor that bridges the two types of denial is clinical documentation quality. Authorization denials that move into retro auth or peer-to-peer review require the clinical record to stand on its own. A payer medical director reviewing the chart for retro authorization approval needs to see clear documentation of medical necessity, the clinical indication, any conservative care attempted, and how the requested service directly impacts diagnosis or treatment decisions.
Billing denials tied to ICD-10 specificity or medical necessity coding require the same foundation. A vague clinical note that does not support the billed diagnosis code is a liability at every stage of the revenue cycle. When documentation is thorough, specific, and tied to functional impact, it supports both the authorization request on the front end and the claim on the back end.
This is why documentation and denial management are not separate conversations for high-performing practices. They are the same conversation.
What This Means for MSOs and Multi-Site Operations
For MSOs managing multiple practice locations, the stakes of denial-type confusion are amplified. A process failure that generates five authorization denials per week at one location may be generating fifty across a ten-site platform. The financial impact scales linearly. The operational complexity of resolving it does not.
MSOs that have implemented centralized denial triage, with clear classification criteria, defined ownership by denial type, and regular denial trend reporting, are better positioned to identify which sites or service lines are underperforming on authorization compliance versus billing accuracy. That specificity allows targeted intervention rather than blanket retraining or process overhaul.
For private equity-backed platforms, denial classification data also matters for financial reporting. Authorization denial rates that exceed industry benchmarks can signal front-end workflow gaps that compress net collections. Billing denial rates that trend upward can indicate coder turnover, payer rule changes, or EHR configuration issues. Neither of those conversations can happen without the data, and the data requires consistent classification from the moment a denial is received.
Practical Next Steps for Practice Leaders
If your practice does not currently have a formal process for classifying denials before resolving them, that is the starting point. It does not require new software. It requires a defined decision rule, clear routing criteria, and team-level accountability for each denial type.
From there, the work is building the upstream processes that prevent each denial category in the first place. For authorization denials, that means a verification and authorization protocol that catches every service requiring prior auth before the patient is seen, with a tracking mechanism that flags expiring authorizations and mismatched CPT codes before claims are submitted. For billing denials, that means regular coding audits, payer-specific modifiers, and billing rule updates, and a quality check on claims before they go out.
None of this is simple to execute at scale. But the practices and MSOs that have built these systems report materially lower denial rates, faster resolution timelines, and more predictable revenue cycle performance across payers and service lines.
DataMatrix Medical supports practice administrators and RCM leaders with prior authorization services, medical billing support, and denial management workflows designed around the distinction that matters most: knowing what kind of denial you have before you try to fix it.
Key Takeaways
- Authorization denials are front-end failures caused by missing, expired, or incorrect authorizations: they should be owned by the prior authorization team, not billing.
- Billing denials are back-end failures caused by coding or data-submission errors: they are resolved within the billing workflow and rarely require the authorization team’s involvement.
- The simplest triage rule: if the EOB mentions authorization, it is a front-end issue; if it mentions coding or data error, it is a billing issue.
- Misclassifying denials wastes staff time, allows retro auth and timely filing windows to close, and leaves recoverable revenue on the table permanently.
- Medical Documentation quality underpins both denial types: a strong clinical note supports the authorization on the front end and the claim on the back end.
- MSOs and multi-site practices benefit most from centralized denial classification data, enabling targeted intervention at the site- or service-line level.
- Building upstream prevention processes, not just resolution workflows, is what separates practices with chronic denial problems from those with manageable, improving denial rates.
Need a Denial Management Partner?
DataMatrix Medical helps practices and MSOs distinguish between authorization and billing failures and build upstream workflows to prevent both.

Nathaniel Smathers is the VP of Client Education and Marketing. He is also a long time contributor of the DataMatrix Medical blog and has a background in healthcare content creation for over a decade. Nathaniel is passionate about exploring the intersections of healthcare, data analysis, and digital innovation.


{kind=link}